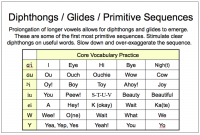
This slide is from my class on improving intelligibility in apraxia, dysarthria, and low cognitive skills. Research has demonstrated that diphthongs and glides are learned very early and that children with phonological impairment rarely have trouble with them. However, it has been my experience that most clients with apraxia, dysarthria, and low cognitive skills do have trouble with them. Typically these children reduce these early sequences down to single vowels, and they often use the schwa instead of the correct vowel. This means that they are…