This advice-column-style blog for SLPs was authored by Pam Marshalla from 2006 to 2015, the archives of which can be explored here. Use the extensive keywords list found in the right-hand column (on mobile: at the bottom of the page) to browse specific topics, or use the search feature to locate specific words or phrases throughout the entire blog.
Diphthongs and Glides in Core Vocabulary Words
By Pam Marshalla
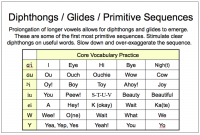
This slide is from my class on improving intelligibility in apraxia, dysarthria, and low cognitive skills. Research has demonstrated that diphthongs and glides are learned very early and that children with phonological impairment rarely have trouble with them. However, it has been my experience that most clients with apraxia, dysarthria, and low cognitive skills do have trouble with them. Typically these children reduce these early sequences down to single vowels, and they often use the schwa instead of the correct vowel. This means that they are…
The Beginnings of “Oral Motor Techniques”
By Pam Marshalla

Q: I’m an undergrad student in my senior year, so my question is for a group project for which I have the history/origins of oral motor exercises. I read your article for the Oral Motor Institute where you reviewed a number of texts. My question is “Is there any name — or names — that are associated with the beginnings of using OMEs? And, are there names associated with bringing it into more mainstream practice? This is all brand new…
Getting Rid of Hypernasality
By Pam Marshalla

Q: My client produces some vowels with nasality. Do you know how to get rid of this problem? Old-fashioned articulation texts (pre-phonology) used to contain large sections, even whole chapters, on how to do this. Let me give you one method to get you started. This one is central to all the rest because it uses a simple biofeedback procedure. Getting rid of nasalization is mostly a matter of ear training. The following represents the way that therapists like Alexander…
Tongue-Protrusion in Toddlers
By Pam Marshalla

Q: I work in the Early Intervention setting and increasingly encounter late talking children (frequently boys) who prefer a frontal tongue posture. What’s the correction? In my experience, this problem does not need to be fixed in a two-year-old boy who is delayed in SL. First, tongue protrusion is normal in two-year-olds. Second, the child is late in talking and therefore should be using the pattern of a one-year-old. The only thing I would do over the next year is…
Working With Fussy or Uncooperative Toddlers
By Pam Marshalla

Q: My toddler-age clients sometimes fuss and cry, even scream. I know this is normal behavior for a little kid, but I am a young therapist with no children of my own yet, and I simply do not know how to handle it. Do you have advice for me? Sometimes it is the language we use that causes stubborn and uncooperative behavior. Changing our language can improve some of these situations. Let me illustrate with a story. 🙂 I was…
Adding Final Schwa
By Pam Marshalla
Q: What about kids who add a schwa to the end or middle of words? Do you have any ideas for that? I see the addition of a schwa as the child’s way of making a simpler speech motor pattern. According to researchers, the CV is the simplest motor pattern and kids change a CVC to a CV-CV to make it easier. All kids do this — e.g., “mom” changes to “mama” and “dad” changes to “dada”. They also do this with the diminutive —…
Global Delays and SL Expectations
By Pam Marshalla

I get questions all the time about children with global delays and severe speech-language impairment. The current trend is to call these children “apraxic” and to treat them like other children with motor speech disorders. But this is an incorrect approach that results in confusion over the purpose and direction of therapy. For example, here is a letter I received lately: I started working with a boy (who is now 3 yrs.) about a year ago. He has delays “across…
Which First: Consonantal or Vocalic R?
By Pam Marshalla

Q: I have read “Successful R Therapy” and am wondering, do you work on Consonantal R or Vocalic R first, and why? I tend to work on Vocalic R with a retroflex R first because I like to teach the contrast between Ah (Jaw low, mouth open, tongue low) with R (jaw high, mouth almost closed, tongue curled up and back). I also find that starting with a big Ah and teaching the client to prolong it helps him hear…
Fixing an Inhaled “S”
By Pam Marshalla

Q: My client breathes in (inhales) on S. How do I fix this? Teach him to exhale and inhale on demand using a straw or other blow toy. Then teach him to exhale and inhale on S. Teach him to hear and appreciate the difference between an inhaled S and an exhaled S. Teach him which one is correct. Practice the exhaled S. Work on syllables, words, and so forth. Also, see my previous post on this topic.
Creating Oral-Nasal Resonance Balance
By Pam Marshalla

Q: My client sounds hypernasal on certain phonemes. How do I work on this? This question is a regular one that comes into my office. It used to be that textbooks on articulation from Van Riper’s era dealt with this topic quite succinctly, but now with our over-focus on phonology and out downplay on all things phonetic, we seem to be forgetting these basic old-time procedures. I will have a chapter of methods on this in my next book, The Marshalla…